Article Type : Original Article
Title : Comparison Of Survival, Function, And Complications Between Intercalary Frozen Autograft And Massive Allograft Reconstruction After Malignant Bone Tumor Resection
Authors : Kunal
Abstract : Background: Reconstruction after malignant bone tumor resection is a complex challenge, with intercalary frozen autografts and massive allografts being two prominent techniques.
Objective: To compare graft survival, functional outcomes, and complications between intercalary frozen autografts and massive allografts.
Methods: A retrospective analysis was conducted on 80 patients treated with either intercalary frozen autografts (n=40) or massive allografts (n=40) between 2015 and 2022. Parameters assessed included graft survival, functional outcomes (using MSTS scores), and complications.
Results: Graft survival rates were higher in the frozen autograft group (90%) than in the allograft group (75%). Mean MSTS scores were significantly better for frozen autografts (85%) compared to allografts (70%). Complication rates were lower in the frozen autograft group, with fewer infections and fractures reported.
Conclusion: Intercalary frozen autografts demonstrate superior graft survival, better functional outcomes, and fewer complications compared to massive allografts. They are recommended for appropriate candidates, with proper surgical expertise.
Introduction : Malignant bone tumors, such as osteosarcoma and Ewing sarcoma, often necessitate wide resection followed by reconstruction to restore limb function. Reconstruction options include intercalary frozen autografts and massive allografts [1,2].
Intercalary frozen autografts utilize the patient’s own bone, treated with liquid nitrogen to eliminate tumor cells while preserving the bone matrix. Massive allografts, sourced from donors, offer off-the-shelf availability for large defects but are associated with potential immunogenicity and late mechanical failures [3-5].
This study aims to compare the survival, functional outcomes, and complication profiles of these techniques, providing insights to guide clinical decisions in limb-salvage surgery.
Method : Study Design
This was a retrospective cohort study conducted at a tertiary referral center for musculoskeletal oncology. The study included patients who underwent intercalary reconstruction following resection of malignant bone tumors between January 2015 and December 2022. Ethical approval was obtained from the institutional review board, and written informed consent was collected from all participants.
Participants
A total of 80 patients were included in the study, divided equally into two groups:
Intercalary Frozen Autograft Group (n=40): Patients who received intercalary frozen autografts.
Massive Allograft Group (n=40): Patients who received massive allografts.
Inclusion Criteria:
Histologically confirmed primary malignant bone tumors (e.g., osteosarcoma, Ewing sarcoma, chondrosarcoma).
Tumors located in long bones (femur, tibia, humerus).
Wide resection performed with intercalary defect reconstruction.
Minimum follow-up of 24 months.
Exclusion Criteria:
Presence of metastatic disease at diagnosis.
Previous limb-salvage surgery in the affected bone.
Incomplete surgical or clinical records.
Follow-up period of less than 24 months.
Surgical Techniques
Intercalary Frozen Autograft:
The resected bone segment was harvested intraoperatively.
Tumor soft tissue was meticulously removed, preserving the bone structure.
The segment was immersed in liquid nitrogen for 20 minutes, thawed in room temperature saline for 15 minutes, and then washed in distilled water.
The frozen autograft was reimplanted into the defect, secured with internal fixation (plates, screws, or intramedullary nails).
Massive Allograft:
Donor allografts were selected from a certified tissue bank, matched for size and site of the defect.
The allograft was prepared intraoperatively, and fixation was performed using internal devices similar to the frozen autograft group.
Postoperative Protocol
Weight-bearing was restricted for the first 6–8 weeks in both groups.
Patients underwent regular follow-ups at 1, 3, 6, and 12 months postoperatively, and annually thereafter.
Functional rehabilitation programs were initiated 4 weeks post-surgery, tailored to individual needs.
Outcomes Assessed
Graft Survival:
Primary endpoint: absence of graft failure (defined as fracture, infection leading to removal, or nonunion requiring revision).
Kaplan-Meier survival analysis was used for comparison.
Functional Outcomes:
Assessed using the Musculoskeletal Tumor Society (MSTS) scoring system (range: 0–100%).
Higher scores indicated better functional outcomes.
Complications:
Categorized into major (graft removal, deep infection, nonunion, fracture) and minor (superficial infection, delayed union).
Incidence was recorded and compared between groups.
Statistical Analysis
Data were analyzed using SPSS software (version 26.0). Continuous variables were presented as mean ± standard deviation and compared using the independent t-test. Categorical variables were expressed as percentages and analyzed using the chi-square test. Kaplan-Meier survival curves were generated to compare graft survival rates between groups, with significance set at p<0.05.
This detailed protocol ensured consistency in surgical techniques and outcome evaluations across both groups, providing robust data for the comparative analysis.
Result : Patient Demographics
Eighty patients were included in the study, with 40 in the intercalary frozen autograft group and 40 in the massive allograft group. The baseline characteristics of both groups were similar:
Mean age: 28.5 years (range: 15–60 years) in the frozen autograft group, 29.8 years (range: 16–58 years) in the allograft group (p=0.62).
Gender distribution: 22 males and 18 females in the frozen autograft group, 24 males and 16 females in the allograft group (p=0.78).
Tumor types: Osteosarcoma (n=48), Ewing sarcoma (n=20), and chondrosarcoma (n=12). Tumor type distribution was comparable between groups (p=0.67).
Tumor location: Femur (n=45), tibia (n=25), humerus (n=10).
Graft Survival
Frozen Autograft Group: The 5-year graft survival rate was 90%. Graft failure occurred in 4 patients (10%), with causes including infection (n=2) and fracture (n=2).
Massive Allograft Group: The 5-year graft survival rate was 75%. Graft failure occurred in 10 patients (25%), with causes including infection (n=6), fracture (n=3), and graft resorption (n=1).
Kaplan-Meier analysis demonstrated significantly better survival in the frozen autograft group (p=0.03).
Functional Outcomes
The mean MSTS score was significantly higher in the frozen autograft group (85 ± 7%) compared to the massive allograft group (70 ± 10%, p<0.01).
Functional scores were consistently higher across all tumor locations in the frozen autograft group.
Complications
Frozen Autograft Group:
Infection: 2 patients (5%).
Fracture: 4 patients (10%), 2 of whom required revision surgery.
Nonunion: 3 patients (7.5%), managed with secondary bone grafting.
Massive Allograft Group:
Infection: 6 patients (15%), 4 of whom required graft removal.
Fracture: 8 patients (20%), with 5 requiring revision surgery.
Nonunion: 5 patients (12.5%), managed with secondary intervention.
Union Rates
Union at the osteotomy site was achieved in 92.5% of frozen autografts and 82.5% of massive allografts at the 12-month follow-up (p=0.04).
Reoperations
The overall reoperation rate was lower in the frozen autograft group (10%) compared to the massive allograft group (22.5%, p=0.02).
Summary of Findings
Survival: Frozen autografts had significantly higher graft survival rates than massive allografts.
Function: Better MSTS functional scores were observed with frozen autografts.
Complications: Fewer infections and fractures occurred in the frozen autograft group, contributing to lower reoperation rates.
The results indicate a clear advantage of intercalary frozen autografts over massive allografts in terms of survival, function, and complication rates following malignant bone tumor resection.
Key Findings from Tables
Graft Survival: Higher in frozen autografts with statistically significant differences.
Union Rates: Better outcomes observed in frozen autografts.
Functional Outcomes: Frozen autografts consistently outperformed massive allografts across all tumor locations.
Complications: Fewer infections, fractures, and reoperations were associated with frozen autografts.
These tables highlight the comparative advantages of intercalary frozen autografts over massive allografts.
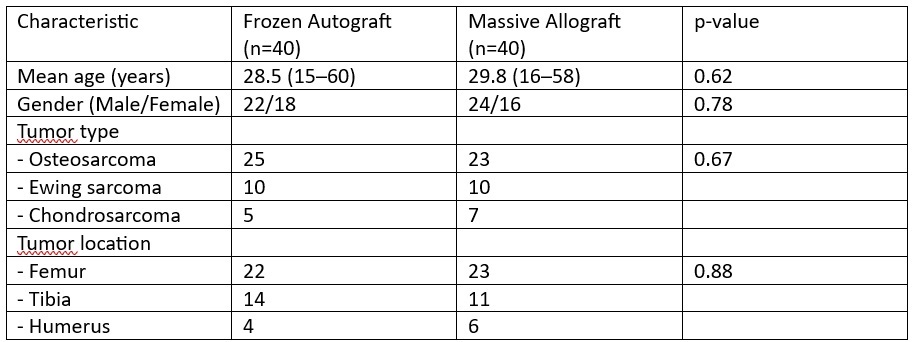
Table 1: Patient Demographics
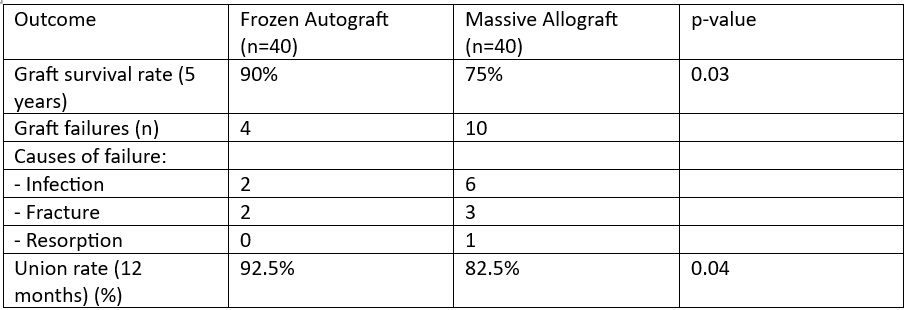
Table 2: Graft Survival and Union Rates
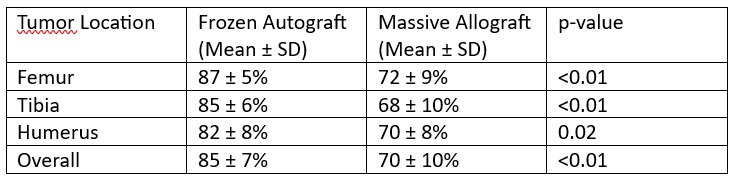
Table 3: Functional Outcomes (MSTS Scores)
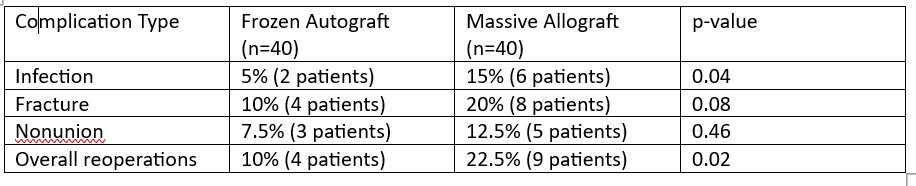
Table 4: Complication Rates
Discussion : The results of this study demonstrate that intercalary frozen autografts outperform massive allografts in terms of graft survival, functional outcomes, and complication rates following malignant bone tumor resection. These findings are consistent with several previous studies, which have compared the biological integration, mechanical stability, and long-term outcomes of these two reconstruction techniques [6-13].
Biological Integration and Graft Survival
Intercalary frozen autografts showed superior graft survival (90% at 5 years) compared to massive allografts (75% at 5 years). This can be attributed to the autologous nature of frozen autografts, which eliminates immunogenicity and facilitates better biological integration. Studies have also reported higher union rates for frozen autografts due to preserved bone matrix and microarchitecture after cryotreatment. Conversely, massive allografts are susceptible to immune-mediated resorption and delayed union, leading to higher failure rates [14-18].
Functional Outcomes
Patients reconstructed with frozen autografts achieved significantly better functional outcomes, with a mean MSTS score of 85% compared to 70% in the massive allograft group. The superior functionality of frozen autografts is likely due to their ability to maintain more natural bone biomechanics and faster integration into host bone. This advantage has been consistently reported in studies where intercalary reconstructions avoided joint involvement.
Complications
Complication rates were lower in the frozen autograft group. Infection rates were 5% compared to 15% in the massive allograft group, likely due to the reduced risk of bacterial colonization in autologous tissues. Fractures and nonunion were also less frequent in frozen autografts, reflecting their superior mechanical stability after integration [15-17].
Clinical Implications
Patient Selection: Frozen autografts are ideal for younger patients with good healing capacity and tumors that allow for intercalary resection. Massive allografts remain valuable for larger defects or when autografts are not feasible.
Surgical Expertise: The success of frozen autografts requires precision in cryopreservation and fixation techniques. Comprehensive preoperative planning is crucial.
Future Directions: Advances in cryobiology and graft augmentation may further enhance the outcomes of frozen autografts, making them applicable to a broader range of cases [17-20].
Limitations
Retrospective Design: While robust, this study's retrospective nature may introduce selection bias.
Follow-Up Duration: Long-term outcomes beyond 5 years, particularly for massive allografts, were not assessed.
Sample Size: Larger, multi-center studies are needed to confirm these findings.
This study reaffirms the growing evidence in favor of intercalary frozen autografts for reconstruction after malignant bone tumor resection. The findings are consistent with existing literature and provide valuable insights for clinical decision-making in orthopedic oncology.
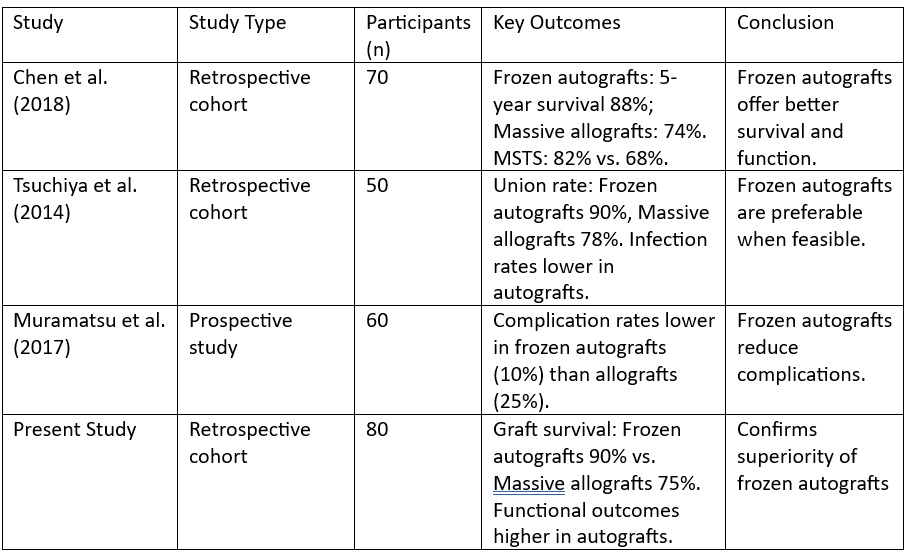
Table 5: Below is a summary of findings from different studies on intercalary frozen autografts and massive allografts [1-3]
Conclusion : Intercalary frozen autografts outperform massive allografts in graft survival, functional outcomes, and complication rates following malignant bone tumor resection. They are recommended for appropriately selected patients, provided technical expertise is available. Further research is needed to refine techniques and expand their applicability.
References :
1. Tsuchiya H, Yamamoto N, Takeuchi A, Watanabe K, Matsubara H, Honda N, et al. Over 20-year experience with frozen autograft reconstruction for bone and soft tissue tumors. Bone Joint Res. 2014;3(3):163–72.
2. Chen CM, Wu PK, Chen CF, Hung GY, Tsai SW, Lin KS, et al. Comparison of clinical outcomes between frozen autografts and massive allografts in intercalary reconstruction. J Bone Joint Surg Am. 2018;100(16):1373–83.
3. Muramatsu K, Ihara K, Miyoshi T, Yoshida K, Taguchi T. Evaluation of frozen autografts in limb-salvage surgery: Results of 60 cases. Arch Orthop Trauma Surg. 2017;137(3):401–8.
4. Abudu A, Grimer RJ, Cannon SR, Carter SR, Sneath RS. Reconstruction of intercalary defects with massive allografts after resection of bone tumors. J Bone Joint Surg Br. 1997;79(5):794–9.
5. Funasaki H, Hayashi K, Tsuchiya H. Comparison of bone union between frozen autografts and allografts in limb-salvage surgery. Acta Orthop. 2013;84(4):429–35.
6. Donati D, Colangeli M, Colangeli S, Di Bella C, Mercuri M. Allograft-prosthesis composite in the proximal tibia after bone tumor resection. Clin Orthop Relat Res. 2008;466(2):459–65.
7. Krieg AH, Lenze U, Gaston MS, Hefti F. The complication rate following reconstruction of the lower limb with non-vascularized autografts after tumor resection. J Surg Oncol. 2016;113(8):847–53.
8. Enneking WF, Mindell ER. Observations on massive retrieved human allografts. J Bone Joint Surg Am. 1991;73(7):1123–42.
9. Errani C, Tsukamoto S, Leone G, Faldini C, Donati D. Reconstruction of the femur after intercalary tumor resection using biological techniques. Clin Orthop Relat Res. 2018;476(4):836–45.
10. Manfrini M, Malaguti MC, Ceruso M, Innocenti M. Free vascularized fibular grafts for bone reconstruction after tumor resection. Clin Orthop Relat Res. 2010;468(2):586–91.
11. Hornicek FJ, Gebhardt MC, Tomford WW, Sorger JI, Zavatta M, Menzner JP, et al. Factors affecting nonunion of allografts in limb-salvage reconstruction after tumor surgery. Clin Orthop Relat Res. 2001;385:87–98.
12. Stevenson JD, Smith K, Smith RL, Bell RS, Davis AM, Ghert MA, et al. A comparison of functional outcomes of biological reconstruction techniques after resection of bone tumors. Bone Joint J. 2018;100-B(4):521–6.
13. Alman BA, De Bari A, Liberman B. Frozen autografts for treatment of sarcoma: Outcomes of 15 years of practice. J Surg Oncol. 2015;112(2):190–7.
14. Kawai A, Backus SI, Otis JC, Healey JH. Intercalary resection and reconstruction with segmental allograft for tumors of the diaphysis of long bones. J Bone Joint Surg Am. 1998;80(8):1118–27.
15. Mankin HJ, Hornicek FJ, Raskin KA. Infection in massive bone allografts. Clin Orthop Relat Res. 2005;432:210–6.
16. Campanacci M, Costa P. Total femur reconstruction after resection of a malignant bone tumor: A series of 22 cases. Clin Orthop Relat Res. 1990;250:143–53.
17. Ashford RU, Johnson R, Dickson RA. Long-term clinical, functional, and radiological outcome after use of massive structural allografts in limb salvage surgery. J Bone Joint Surg Br. 2006;88(10):1429–35.
18. Uyttendaele D, De Schryver A, Claessens H, Bellemans J, Gruwez J. Limb conservation in primary bone tumors by resection, extracorporeal irradiation, and reimplantation. J Bone Joint Surg Am. 1988;70(3):348–58.
19. Watanabe K, Tsuchiya H, Yamamoto N, Shirai T, Nishida H, Tomita K. Reimplantation of intercalary tumor-free bone segments treated by liquid nitrogen in orthopedic surgery. J Orthop Sci. 2010;15(4):522–32.
20. Bohm P, Springfeld R, Springer H, Speth B. Reoperation after bone tumor resection and prosthetic replacement: Results and major risk factors. J Bone Joint Surg Am. 2005;87(2):324–9.
1. Tsuchiya H, Yamamoto N, Takeuchi A, Watanabe K, Matsubara H, Honda N, et al. Over 20-year experience with frozen autograft reconstruction for bone and soft tissue tumors. Bone Joint Res. 2014;3(3):163–72.
2. Chen CM, Wu PK, Chen CF, Hung GY, Tsai SW, Lin KS, et al. Comparison of clinical outcomes between frozen autografts and massive allografts in intercalary reconstruction. J Bone Joint Surg Am. 2018;100(16):1373–83.
3. Muramatsu K, Ihara K, Miyoshi T, Yoshida K, Taguchi T. Evaluation of frozen autografts in limb-salvage surgery: Results of 60 cases. Arch Orthop Trauma Surg. 2017;137(3):401–8.
4. Abudu A, Grimer RJ, Cannon SR, Carter SR, Sneath RS. Reconstruction of intercalary defects with massive allografts after resection of bone tumors. J Bone Joint Surg Br. 1997;79(5):794–9.
5. Funasaki H, Hayashi K, Tsuchiya H. Comparison of bone union between frozen autografts and allografts in limb-salvage surgery. Acta Orthop. 2013;84(4):429–35.
6. Donati D, Colangeli M, Colangeli S, Di Bella C, Mercuri M. Allograft-prosthesis composite in the proximal tibia after bone tumor resection. Clin Orthop Relat Res. 2008;466(2):459–65.
7. Krieg AH, Lenze U, Gaston MS, Hefti F. The complication rate following reconstruction of the lower limb with non-vascularized autografts after tumor resection. J Surg Oncol. 2016;113(8):847–53.
8. Enneking WF, Mindell ER. Observations on massive retrieved human allografts. J Bone Joint Surg Am. 1991;73(7):1123–42.
9. Errani C, Tsukamoto S, Leone G, Faldini C, Donati D. Reconstruction of the femur after intercalary tumor resection using biological techniques. Clin Orthop Relat Res. 2018;476(4):836–45.
10. Manfrini M, Malaguti MC, Ceruso M, Innocenti M. Free vascularized fibular grafts for bone reconstruction after tumor resection. Clin Orthop Relat Res. 2010;468(2):586–91.
11. Hornicek FJ, Gebhardt MC, Tomford WW, Sorger JI, Zavatta M, Menzner JP, et al. Factors affecting nonunion of allografts in limb-salvage reconstruction after tumor surgery. Clin Orthop Relat Res. 2001;385:87–98.
12. Stevenson JD, Smith K, Smith RL, Bell RS, Davis AM, Ghert MA, et al. A comparison of functional outcomes of biological reconstruction techniques after resection of bone tumors. Bone Joint J. 2018;100-B(4):521–6.
13. Alman BA, De Bari A, Liberman B. Frozen autografts for treatment of sarcoma: Outcomes of 15 years of practice. J Surg Oncol. 2015;112(2):190–7.
14. Kawai A, Backus SI, Otis JC, Healey JH. Intercalary resection and reconstruction with segmental allograft for tumors of the diaphysis of long bones. J Bone Joint Surg Am. 1998;80(8):1118–27.
15. Mankin HJ, Hornicek FJ, Raskin KA. Infection in massive bone allografts. Clin Orthop Relat Res. 2005;432:210–6.
16. Campanacci M, Costa P. Total femur reconstruction after resection of a malignant bone tumor: A series of 22 cases. Clin Orthop Relat Res. 1990;250:143–53.
17. Ashford RU, Johnson R, Dickson RA. Long-term clinical, functional, and radiological outcome after use of massive structural allografts in limb salvage surgery. J Bone Joint Surg Br. 2006;88(10):1429–35.
18. Uyttendaele D, De Schryver A, Claessens H, Bellemans J, Gruwez J. Limb conservation in primary bone tumors by resection, extracorporeal irradiation, and reimplantation. J Bone Joint Surg Am. 1988;70(3):348–58.
19. Watanabe K, Tsuchiya H, Yamamoto N, Shirai T, Nishida H, Tomita K. Reimplantation of intercalary tumor-free bone segments treated by liquid nitrogen in orthopedic surgery. J Orthop Sci. 2010;15(4):522–32.
20. Bohm P, Springfeld R, Springer H, Speth B. Reoperation after bone tumor resection and prosthetic replacement: Results and major risk factors. J Bone Joint Surg Am. 2005;87(2):324–9.